Background
Prostate cancer (PCa) is 1 of the most common types of cancer in adult men, with an estimated 299 010 new diagnoses and 35 250 deaths in 2024 in the United States.1 Only 5% to 10% of all patients with PCa are diagnosed with metastatic disease, and metastatic PCa is responsible for 50% of all PCa-related deaths.2 Androgen-deprivation therapy (ADT) is the cornerstone treatment for metastatic hormone-sensitive PCa (mHSPC),3 and augmenting ADT with chemotherapy or novel androgen receptor synthesis inhibitors (ARSIs) has increased patient survival.4 Despite these substantial advances in systemic treatment, mHSPC remains a challenge because patients will eventually develop castration resistance, which limits their systemic treatment options.
The role of radiation therapy (RT) to the primary tumor in the setting of mHSPC continues to be an area of active investigation. Current guidelines now recommend RT to the primary tumor as standard of care for patients with de novo mHSPC and low metastatic burden on the basis of results from the Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy (STAMPEDE) trial.3,5 Treatment selection is still based solely on tumor burden, however, as assessed by conventional imaging. Several efforts have been made to tailor systemic treatment for patients with metastatic PCa, such as the identification of specific therapeutic targets through germline and somatic testing and the development of targeted therapies.6,7 Data supporting the role of molecular testing and genetic profiling in patients with metastatic PCa who could benefit from RT to the primary tumor remain scarce.2,8
Here, we present the case of a man diagnosed with low-volume mHSPC with substantial somatic mutations and tumor mutation burden (TMB). The patient gave written informed consent before the publication of this article.
Abbreviations
ADT androgen deprivation therapy
ARSIandrogen receptor synthesis inhibitor
mCRPC metastatic castration-resistant prostate cancer
mHSPC metastatic hormone-sensitive prostate cancer
SWOG Southwest Oncology Group
MRI magnetic resonance imaging
OS overall survival
PCa prostate cancer
PORTOS Post-Operative Radiation Therapy Outcomes Score
PSA prostate-specific antigen
PSMA prostate-specific membrane antigen
RT radiation therapy
STAMPEDE Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy
TMB tumor mutation burden
Case Report
The patient is a 68-year-old Latino man with a history of mild cognitive impairment. He initially presented to the emergency department with substantial rectal pain and bleeding in late 2022. In early 2023, a computed tomographic scan of the patient’s abdomen and pelvis revealed a perirectal mass measuring 3.7 × 5.0 × 4.9 cm. This mass was later confirmed by colonoscopy to occupy approximately 50% of the circumference of the distal rectum and anal canal. Subsequent biopsy of the mass confirmed high-grade adenocarcinoma of the prostate, with a Gleason score of 10 (5 + 5). Magnetic resonance imaging (MRI) of the pelvis revealed the full extent of the mass, which measured 6.1 × 7.1 × 8.1 cm and involved the posterior half of the prostate gland, the rectal wall, and the rectal prostatic space. Several enlarged lymph nodes were observed in varying locations of the pelvis and lower abdomen, including an external iliac lymph node measuring 3.5 × 2.3 × 2.1 cm and multiple inguinal lymph nodes (Figure 1A). Piflufolastat fluorine-18 prostate-specific membrane antigen (PSMA) positron emission tomography imaging showed PSMA avidity in the primary tumor and in the aforementioned enlarged lymph nodes. The PSMA avidity did not suggest the presence of osseous or visceral metastases (Figure 1B). Disease staging per American Joint Committee on Cancer, version 8, was finalized as stage IVb (cT4b, cN1, cM1) de novo, low-volume mHSPC.
First-line treatment with ADT and an androgen receptor inhibitor, darolutamide, was promptly initiated. A follow-up pelvic MRI scan after 3 months showed an initial response to treatment, with a substantial decrease in the size of the prostate gland (3.0 × 1.8 × 4.0 cm) and lymph nodules, including the external iliac lymph nodule (2.7 × 0.9 cm), but disease involvement in the rectal wall persisted. In mid-2023, after 4 months of ADT, the patient’s prostate-specific antigen (PSA) serum levels rose from 1.12 µg/L
(ng/mL) to 2.15 µg/L within 4 weeks, indicating early castration resistance. An additional MRI scan after 6 months of ADT revealed a substantial increase in the size of the perirectal mass (4.7 × 3.4 × 6.5 cm), a mild increase in the size of the iliac nodal metastasis, and new mesorectal and presacral nodules. Next-generation sequencing of the pretreatment sample of the primary tumor revealed the presence of a considerable number of missense and stop-gain alterations in actionable target genes and a high TMB, with 21 alterations per megabase. These genes include ATM, BAP1, FLT3, MSH6, NF1, PTEN, RB1, SPOP, TP53, and JAK1 (see Supplemental Figure 1, available online).
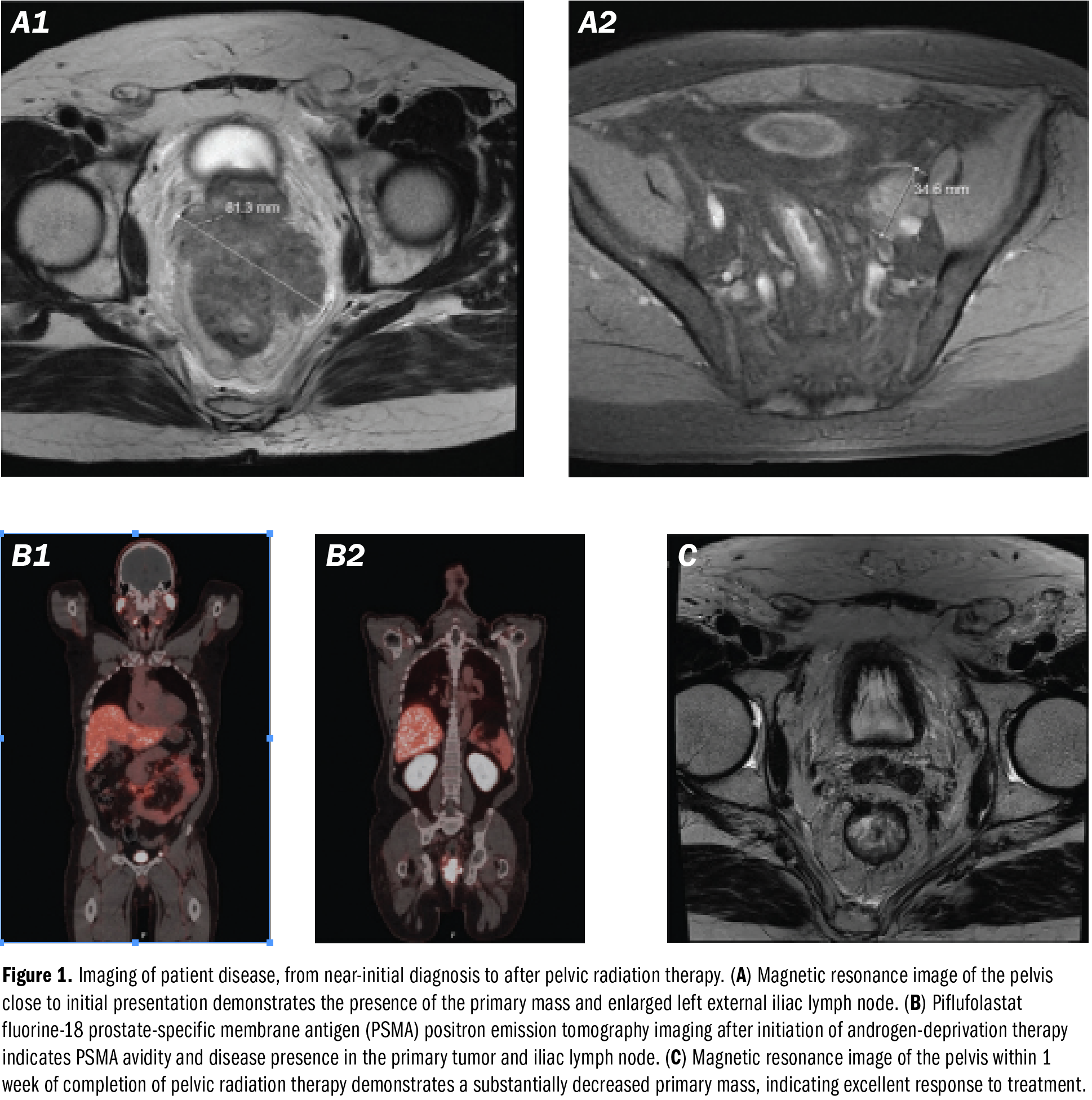
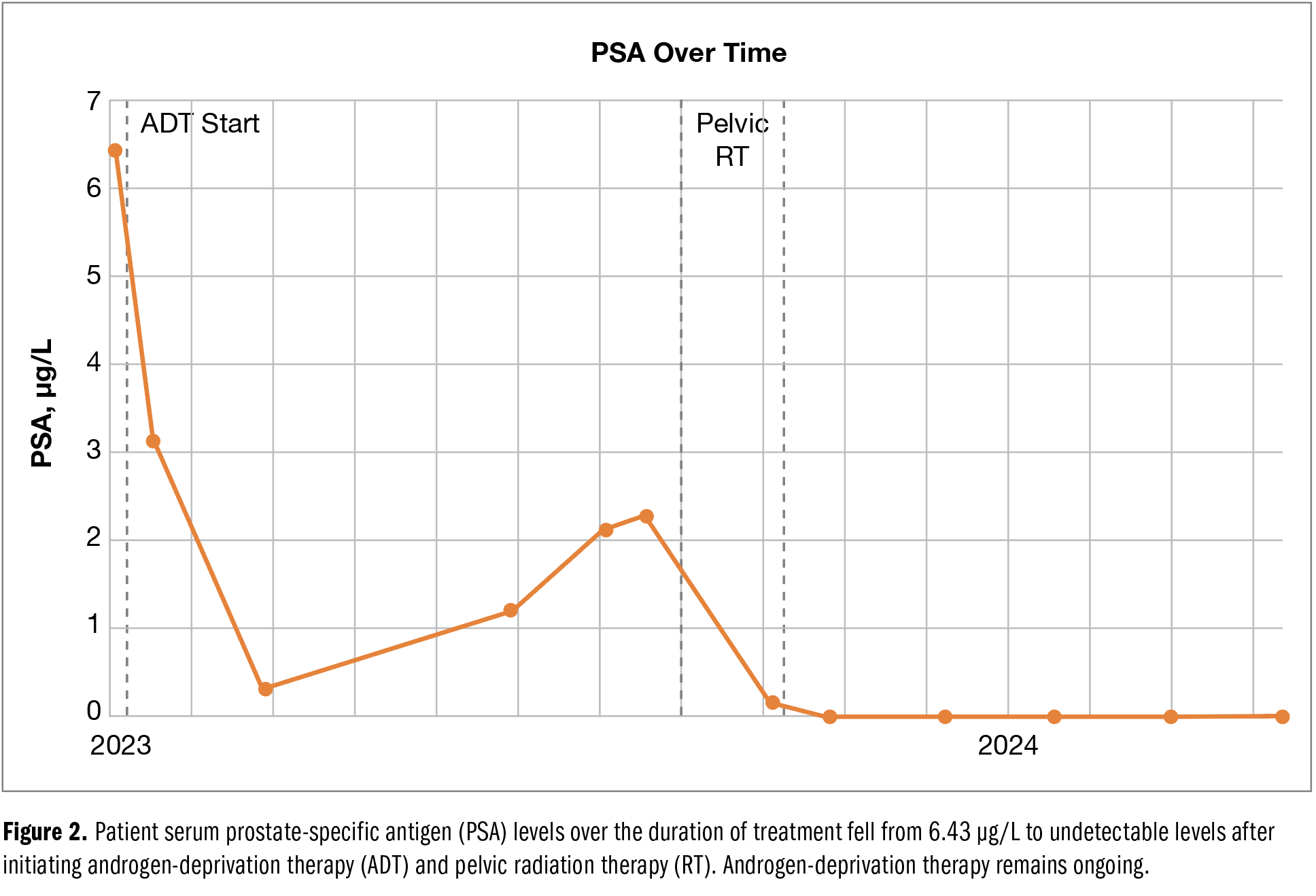
Given the increase in PSA levels, despite an initial response to treatment, a course of pelvic external beam RT was initiated to maintain local disease control. The patient received 45 Gy in 25 fractions to the pelvis, followed by an additional 24-Gy boost dose in 8 fractions (total dose of 69 Gy) to the prostate, seminal vesicles, and rectal mass. The patient completed RT in late 2023 with no major adverse events noted. In the month following external beam RT, serum PSA levels declined to undetectable levels (Figure 2). Subsequent MRI scans revealed a further substantial decrease in the rectal component, now measuring 3.0 × 1.5 cm compared with the previously measured 4.7 × 3.4 cm (Figure 1C). Iliac and femoral lymphadenopathy also saw substantial improvement, with both nodes measuring 1.0 cm or smaller. More notably, the patient reported substantial improvement of his rectal pain and bleeding. As of early 2024, the patient has continued receiving ADT and darolutamide, with undetectable serum PSA levels and minimal lasting complications related to treatment.
Discussion
We report the case of a patient with newly diagnosed, low-volume mHSPC who initially developed early castration resistance and received RT to the primary tumor, with partial radiologic response and complete biochemical response. After 8 months, the patient has remained without disease progression. On somatic testing, the patient’s disease had a high TMB, high microsatellite instability, and a missense alteration in ATM and other genes that may suggest remarkable response to treatment.
Evidence increasingly supports the role of RT in the treatment of primary tumors in patients with mHSPC, but this area remains a subject of investigation, and opting for RT to the primary tumor should be based on clinical characteristics and individual patient selection. A large registry study using the National Cancer Database reported a statistically significant increase in overall survival (OS) in patients with mHSPC who received RT to the primary tumor in addition to ADT.9 The HORRAD trial10 was the first clinical trial to randomly assign patients with mHSPC to receive ADT with or without RT to the primary tumor. The trial did not, however, demonstrate an improvement in OS in patients receiving RT. Notably, there was a trend toward better OS in patients with 5 or fewer bone lesions who received RT to the primary tumor.10 Following that trial, arm H of the STAMPEDE trial demonstrated that RT to the primary tumor, in addition to ADT, improved OS in patients with mHSPC and a low metastatic burden, defined as fewer than 4 bone metastases and no visceral involvement.11 Recently, the Phase III Study for Patients With Metastatic Hormone-naïve Prostate Cancer (PEACE1) trial evaluated the role of adding RT to the primary tumor in patients receiving systemic treatment with a triplet regimen of ADT, abiraterone, and docetaxel. In this trial, adding RT to the primary tumor did not improve OS but did reduce severe urinary symptoms.12 Effect of Statins on Oxidative Stress and Endothelial Progenitor Cells (STOPCAP),13 a meta-analysis that used patient data obtained across the STAMPEDE, HORRAD, and PEACE1 trials to examine the role of prostate RT for patients with mHSPC, reinforced these findings. The meta-analysis found that OS and progression-free survival did not improve in patients with low metastatic burden who received RT; however, in congruence with previous data, a statistically significant improvement was noted in time to biochemical progression and failure-free survival. Additional analysis showed a 7% improvement in 3-year survival in patients with fewer than 5 bone metastases.13 Regarding ongoing investigations for the role of RT in metastatic PCa, the Southwest Oncology Group’s SWOG-1802 trial14 is an ongoing phase 3 trial investigating the role of definitive treatment, including prostatectomy and RT, alongside standard systemic treatment (ie, combination ADT and ARSI) for patients with de novo metastatic PCa.
In addition, preclinical evidence has pointed to a synergistic effect of RT with ARSIs in PCa cells, showing decreased cell viability with increased DNA strand breaks compared with control patients who did not receive RT.15 In the clinical setting, the STAMPEDE trial proved the synergistic effect of concomitant ADT with an ARSI in combination with RT in patients with high-risk nonmetastatic PCa, including node-positive disease.16
Analysis of tumor suppressor genes as potential prognostic gene expression signatures in the setting of mHSPC from the Chemohormonal Therapy Versus Androgen Ablation Randomized Trial for Extensive Disease in Prostate Cancer (CHAARTED) trial suggests that somatic mutations in RB1, PTEN, and TP53 are correlated with adverse outcomes when treated solely with ADT with or without docetaxel.17 Furthermore, long-term follow-up and analysis of potential genetic predictors from the Surveillance or metastasis-directed Therapy for OligoMetastatic Prostate cancer recurrence (STOMP) and Observation versus Stereotactic Ablative Radiation for OLigometastatic Prostate CancEr (ORIOLE) trials revealed that carrying somatic mutations in ATM, BRCA1/2, RB1, or TP53 indicated a more statistically significant sustained clinical benefit in response to metastasis-directed RT for patients with oligometastatic PCa vs patients without these alterations.18
The use of precision medicine to predict the benefit of RT in patients with metastatic PCa has not been conclusively established in clinical practice. This gap is primarily attributed to the limited availability of clinical evidence, a lack of consensus, associated costs, and overall feasibility.19 Currently, specific efforts are being made only to integrate molecular testing to predict the benefit of RT. The Post-Operative Radiation Therapy Outcomes Score (PORTOS) is a predictive signature of distant metastasis risk after RT that was developed by incorporating the expression of 24 genes.20 In a validation cohort, patients treated with RT had a decreased incidence of distant metastases within the high PORTOS group but not the low PORTOS group, providing a proof of concept for the integration of molecular markers within a selection of patients who could benefit from RT in addition to systemic therapy.20
Several gene signatures have been identified in the setting of localized PCa that correlate to more aggressive localized disease, progression to metastatic disease, and radiation resistance. Thangavel and colleagues21 determined that the loss of a functional RB gene resulted in enhanced radiation sensitivity in multiple hormone-sensitive and hormonal-resistant PCa cell lines. Further analysis by Thangavel indicated that a loss of function in RB in murine models promoted a disease phenotype that is substantially more susceptible to metastatic progression.22 Loss of PTEN has also been associated with an increased likelihood of metastatic progression and resistance to androgen deprivation and chemotherapies, with as many as 50% of castration-resistant tumors being PTEN deficient.23 In a postprostatectomy setting, alterations in ERG resulting in negative expression were strongly associated with immediate progression; a similar trend was noted in patients with aberrant PTEN expression.24 Clinical validation for the use of these genes as predictive biomarkers remains sparse, especially in the setting of metastatic disease. Preliminary clinical and preclinical models examining these genes and others have shown promise regarding their prognostic capability for disease progression and therapeutic response in PCa. Further validation of these single and multigene prognostic indicators in patients within clinical setting is vital.
In the setting of metastatic castration-resistant PCa (mCRPC), exploratory studies investigating the use of radiopharmaceutical therapies, such as radium-223 or PSMA-directed radioligand therapies, have shown marked differences between patients with different somatic mutations. For example, an exploratory study by Isaacsson Velho and colleagues25 showed that patients with mCRPC and bony metastatic disease had statistically significantly better responses and longer time to progression while receiving radium-223 if they possessed germline or somatic alterations in genes involved in the homologous repair pathway (eg, BRCA2, ATM, ATR). In a study supplementing the Study of 177Lu-PSMA-617 In Metastatic Castrate-Resistant Prostate Cancer (VISION) trial that investigated the use of lutetium-177-PSMA-617 radioligand therapy in mCRPC, patients with gain-of-function alterations in plasma androgen receptor genes demonstrated greater susceptibility to earlier disease progression and lower OS.26 Existing clinical and preclinical evidence in external beam and radiopharmaceutical therapies indicates a growing need for the integration of precision medicine and genomics when evaluating a patient with PCa and their treatment needs.
The profound response of this patient’s tumor to RT in the context of its initially middling response to ADT and darolutamide provides some evidence for the integration of precision medicine in the context of metastatic PCa and evaluation for RT. Castration resistance currently presents a massive obstacle in the long-term management of metastatic PCa, and greater adoption of precision medicine could provide the means to reduce reliance on ADT and ARSIs alone for long-term disease management. The basis for using precision medicine has already been laid in the context of metastatic PCa, with the US Food and Drug Administration having already approved the use of poly(ADP-ribose) polymerase inhibitors in mCRPC. Disease management through poly(ADP-ribose) polymerase inhibitors largely relies on observing somatic deficiencies in homologous recombination repair genes, such as BRCA1/2.27
Conclusion
We speculate that in this patient, high TMB, alongside other associated factors, may have played a role in the complete response to RT to the primary tumor after indication of early castration resistance. Although precision medicine in oncology has grown substantially in recent years, its scope remains limited. Genomic and transcriptomic sequencing analysis has been more frequently adopted for systemic treatment selection in patients with cancer, although adoption of this rapidly evolving technology is not yet universal in all areas of oncology. Although little pretext has been established in the literature, we believe that this case emphasizes the importance of expanding precision medicine in the context of metastatic PCa and highlights the potential role of RT in local control and overall disease management.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763
2. Piombino C, Oltrecolli M, Tonni E, et al. De novo metastatic prostate cancer: are we moving toward a personalized treatment? Cancers (Basel). 2023;15(20):4945. doi:10.3390/cancers15204945
3. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Prostate cancer version 4.2024. May 17, 2024. Accessed September 25, 2024. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
4. Sayegh N, Swami U, Agarwal N. Recent advances in the management of metastatic prostate cancer. JCO Oncol Pract. 2022;18(1):45-55. doi:10.1200/OP.21.00206
5. Parker C, Castro E, Fizazi K, et al. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(9):1119-1134. doi:10.1016/j.annonc.2020.06.011
6. De Bono J, Mateo J, Fizazi K, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2020;382(22):2091-2102. doi:10.1056/NEJMoa1911440
7. Fizazi K, Piulats JM, Reaume MN, et al. Rucaparib or physician’s choice in metastatic prostate cancer. N Engl J Med. 2023;388(8):719-732. doi:10.1056/NEJMoa2214676
8. Tam A, Mercier BD, Thomas RM, et al. Moving the needle forward in genomically-guided precision radiation treatment. Cancers. 2023;15(22):5314. doi:10.3390/cancers15225314
9. Rusthoven CG, Jones BL, Flaig TW, et al. Improved survival with prostate radiation in addition to androgen deprivation therapy for men with newly diagnosed metastatic prostate cancer. J Clin Oncol. 2016;34(24):2835-2842. doi:10.1200/JCO.2016.67.4788
10. Boevé LMS, Hulshof MCCM, Vis AN, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial: data from the HORRAD trial. Eur Urol. 2019;75(3):410-418. doi:10.1016/j.eururo.2018.09.008
11. Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018;392(10162):2353-2366. doi:10.1016/S0140-6736(18)32486-3
12. Bossi A, Foulon S, Maldonado X, et al. Prostate irradiation in men with de novo, low-volume, metastatic, castration-sensitive prostate cancer (mCSPC): results of PEACE-1, a phase 3 randomized trial with a 2x2 design. J Clin Oncol. 2023;41(17_suppl):LBA5000. doi:10.1200/JCO.2023.41.17_suppl.LBA5000
13. Burdett S, Boevé LM, Ingleby FC, et al. Prostate radiotherapy for metastatic hormone-sensitive prostate cancer: a STOPCAP systematic review and meta-analysis. Eur Urol. 2019;76(1):115-124. doi:10.1016/j.eururo.2019.02.003
14. Standard systemic therapy with or without definitive treatment in treating participants with metastatic prostate cancer. ClinicalTrials.gov identifier: NCT03678025. Updated August 16, 2024. Accessed November 9, 2024. https://clinicaltrials.gov/study/NCT03678025
15. Wright TC, Dunne VL, Alshehri AHD, Redmond KM, Cole AJ, Prise KM. Abiraterone in vitro is superior to enzalutamide in response to ionizing radiation. Front Oncol. 2021;11:700543. doi:10.3389/fonc.2021.700543
16. Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022;399(10323):447-460. doi:10.1016/S0140-6736(21)02437-5
17. Jiménez N, Garcia de Herreros M, Reig Ò, et al. Development and independent validation of a prognostic gene expression signature based on RB1, PTEN, and TP53 in metastatic hormone-sensitive prostate cancer patients. Eur Urol Oncol. 2024;7(4):954-964. doi:10.1016/j.euo.2023.12.012
18. Deek MP, Van der Eecken K, Sutera P, et al. Long-term outcomes and genetic predictors of response to metastasis-directed therapy versus observation in oligometastatic prostate cancer: analysis of STOMP and ORIOLE trials. J Clin Oncol. 2022;40(29):3377-3382. doi:10.1200/JCO.22.00644
19. Cussenot O, Cancel-Tassin G, Rao SR, et al. Aligning germline and somatic mutations in prostate cancer. Are genetics changing practice? BJU Int. 2023;132(5):472-484. doi:10.1111/bju.16120
20. Zhao SG, Chang SL, Spratt DE, et al. Development and validation of a 24-gene predictor of response to postoperative radiotherapy in prostate cancer: a matched, retrospective analysis. Lancet Oncology. 2016;17(11):1612-1620. doi:10.1016/S1470-2045(16)30491-0
21. Thangavel C, Boopathi E, Ciment S, et al. The retinoblastoma tumor suppressor modulates DNA repair and radioresponsiveness. Clin Cancer Res. 2014;20(21):5468-5482. doi:10.1158/1078-0432.CCR-14-0326
22. Thangavel C, Boopathi E, Liu Y, et al. RB loss promotes prostate cancer metastasis. Cancer Res. 2017;77(4):982-995. doi:10.1158/0008-5472.CAN-16-1589
23. Jamaspishvili T, Berman DM, Ross AE, et al. Clinical implications of PTEN loss in prostate cancer. Nat Rev Urol. 2018;15(4):222-234. doi:10.1038/nrurol.2018.9
24. Brady L, Carlsson J, Baird AM, et al. Correlation of integrated ERG/PTEN assessment with biochemical recurrence in prostate cancer. Cancer Treat Res Commun. 2021;29:100451. doi:10.1016/j.ctarc.2021.100451
25. Isaacsson Velho P, Qazi F, Hassan S, et al. Efficacy of radium-223 in bone-metastatic castration-resistant prostate cancer with and without homologous repair gene defects. Eur Urol. 2019;76(2):170-176. doi:10.1016/j.eururo.2018.09.040
26. De Giorgi U, Sansovini M, Severi S, et al. Circulating androgen receptor gene amplification and resistance to 177Lu-PSMA-617 in metastatic castration-resistant prostate cancer: results of a Phase 2 trial. Br J Cancer. 2021;125(9):1226-1232. doi:10.1038/s41416-021-01508-5
27. Taylor AK, Kosoff D, Emamekhoo H, Lang JM, Kyriakopoulos CE. PARP inhibitors in metastatic prostate cancer. Front Oncol. 2023;13:1159557. doi:10.3389/fonc.2023.1159557
Article Information
Published: December 13, 2024.
Conflict of Interest Disclosures: The authors have nothing to disclose.
Funding/Support: This study did not receive external funding.
Author Contributions: Concept and design: B.M., R.B.C., and Y.R.L. Drafting of the article: B.M. and R.B.C. Critical review of the manuscript for important intellectual content: A. Ta., D.C., S.J.C., A.Tr., Y.R.L., and R.B.C. Administrative, technical, or material support: B.M., R.B.C., and Y.R.L. Supervision: R.B.C., A.Ta., A.Tr., and Y.R.L.
Data Availability Statement: The data supporting the findings of this clinical case are available from the corresponding author upon request, subject to consideration of ethics and patient privacy.